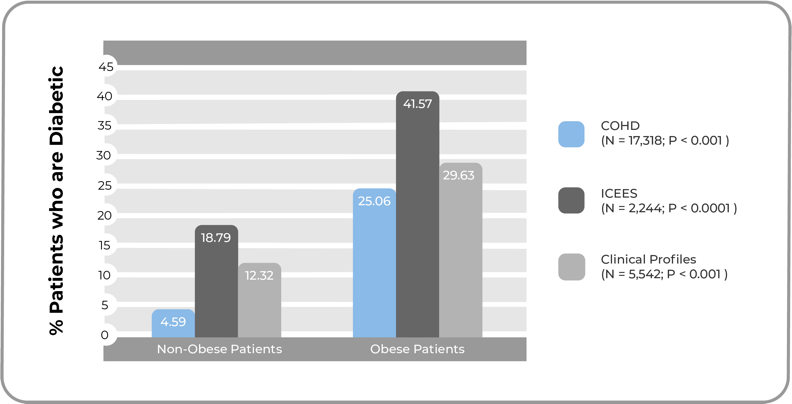

Clinical Profiles
Represents statistical profiles of disease, including data on demographics, diagnoses and disease comorbidities, laboratory tests, procedures, and medications; derived from observational patient data collected by Johns Hopkins Medicine.
COHD
An open clinical database including counts and frequencies of conditions, procedures, drug exposures and patient demographics derived from the Columbia University Medical Center’s Observational Health Data Sciences and Informatics (OHDSI) database.
ICEES
A complex extraction, conversion and integration pipeline, derived from the UNC Health Care System, that integrates clinical and exposures data while keeping the data openly accessible.
ROBOKOP
A reasoning tool created for Translator that uses data from myriad open databases to make connections between seemingly unrelated data points.